Skip to content
What is the PUJ?
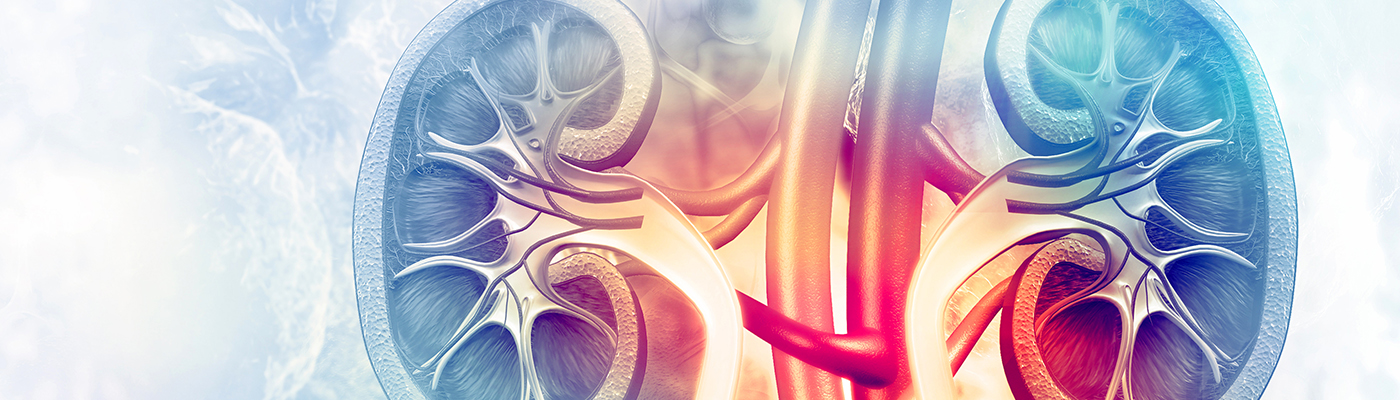
- To understand what the PUJ is, requires some basic anatomical back ground information.
- The kidney acts as a filter, filtering the blood with the excreted waste product being the urine. The urine collects within the collecting system of the kidney (calyces and renal pelvis).
- The central renal pelvis drains into a tube (ureter) which drains all the way down to the bladder.
- The PUJ is the point at which the renal pelvis joins the ureter.
What is a PUJ obstruction?
- A PUJ obstruction is where there is an obstruction to normal urine flow from the renal pelvis into the ureter.
- It may be classified as either:
- Congenital/primary – essentially present since birth as a developmental abnormality. The cause of congenital PUJ obstruction is incompletely understood but may be as a result of abnormal insertion of the ureter into the renal pelvis, abnormal arrangement of ureteric musculature at the PUJ or a crossing vessel (usually artery) running in front of the PUJ causing an obstruction.
- Acquired/secondary – this type of narrowing (stricture) may have resulted from previous surgery/instrumentation, kidney stones or trauma
What are the symptoms of a PUJ obstruction?
- The classic symptoms of a PUJ obstruction are:
- Flank pain – often worsened after consuming large volumes of fluids, especially alcohol
- Recurrent urinary tract infections
- Blood in urine (haematuria)
- Rarely, the swollen/obstructed kidney can be felt in the flank region
How are PUJ obstructions diagnosed?
- In some cases, a PUJ obstruction will be detected due to the presence of the above symptoms, resulting in further investigations which reveal the PUJ obstruction
- Frequently, a PUJ obstruction will be detected incidentally on ultrasound or CT scans. A PUJ obstruction has a typical appearance on CT scan, however not all patients with this appearance will have obstruction to the urine flow. It is only patients which have a physical obstruction that require treatment.
What tests will be required to determine if a PUJ obstruction is significant?
- A history and examination will determine if symptoms and signs exist suggesting an obstruction
- Baseline tests required include:
- Urine culture – to exclude a urine tract infection
- Blood tests – to check baseline kidney function
- CT Urogram/IVP – is a dedicated CT scan of the kidneys and ureter with intravenous contrast. It provides anatomical information to help determine if a true PUJ obstruction exists
- Mag 3 scan – this specialised nuclear medicine scan is critical to determine if a true obstruction to kidney drainage exists. It will also provide a split function of the kidneys (i.e. what percentage of total kidney function each kidney is providing)
- Cystoscopy/ Ureteroscopy – this is not required in all cases. Particularly in suspected acquired cases, a telescopic inspection of the PUJ will be required to determine the length of narrowing and to exclude any other pathology (e.g. stone or malignancy)
Do all PUJ obstructions require treatment?
- All true PUJ obstructions require treatment, however as mentioned, not all patients with the appearance of a PUJ obstruction have significant obstruction.
- Those that require treatment include:
- Symptomatic obstruction (see above)
- Impaired kidney function with obstruction
- Reduced split function of affected kidney or falling split function on follow up scans (usually >10% difference between kidneys)
- Recurrent urinary tract infections
- Formers of kidney stones
- Evidence of obstruction on Mag 3 scan – however, elderly patients or those with multiple medical problems may not require treatment
What are the treatment options for PUJ obstruction?
- Surgery is the mainstay of treatment for a PUJ obstruction.
- The gold standard is a pyeloplasty (for details see urological procedures explained)
- A pyeloplasty is usually performed with key hole surgery (laparoscopic)
- It involves cutting out the narrowed/obstructed PUJ segment and re-joining the ureter to the renal pelvis with sutures in such a way to allow unimpeded drainage
- A ureteric stent will be left in the ureter for 6 weeks
- The operation is successful in >90-95% cases
- A Mag 3 scan will be performed 3 month after the Pyeloplasty to ensure unobstructed drainage
- Endopyelotomy – is a minimally invasive surgical option for treating PUJ obstruction. It involves the passage of a fine telescope (ureteroscope) to the PUJ and the use of a laser to cut the stricture/narrowing along its length. A stent will be left in for 4- 6 weeks. It is less effective than a pyeloplasty in both the short and long term. Success rates range between 60-80%. For that reason it is not recommended as the first line option for a PUJ obstruction. It may be used in cases of a failed pyeloplasty with reasonable success.
- Ureteric stent – long term. For some elderly patients with a significant PUJ obstruction that require treatment but are not fit enough to tolerate a pyeloplasty, a long term ureteric stent may be an appropriate option. This will need to be changed very 6-12 months